
Tairāwhiti data, 22 September 2023
Tairāwhiti data, 22 September 2023
Covid low; Typhoid cluster source; Leptospirosis tests
Covid-19 cases in Tairāwhiti continue to fall reaching new lows: 20 cases for the week ending 21 September; 29 for the previous week. The 7-day average fell to 2.9 from 4.1 the previous week.
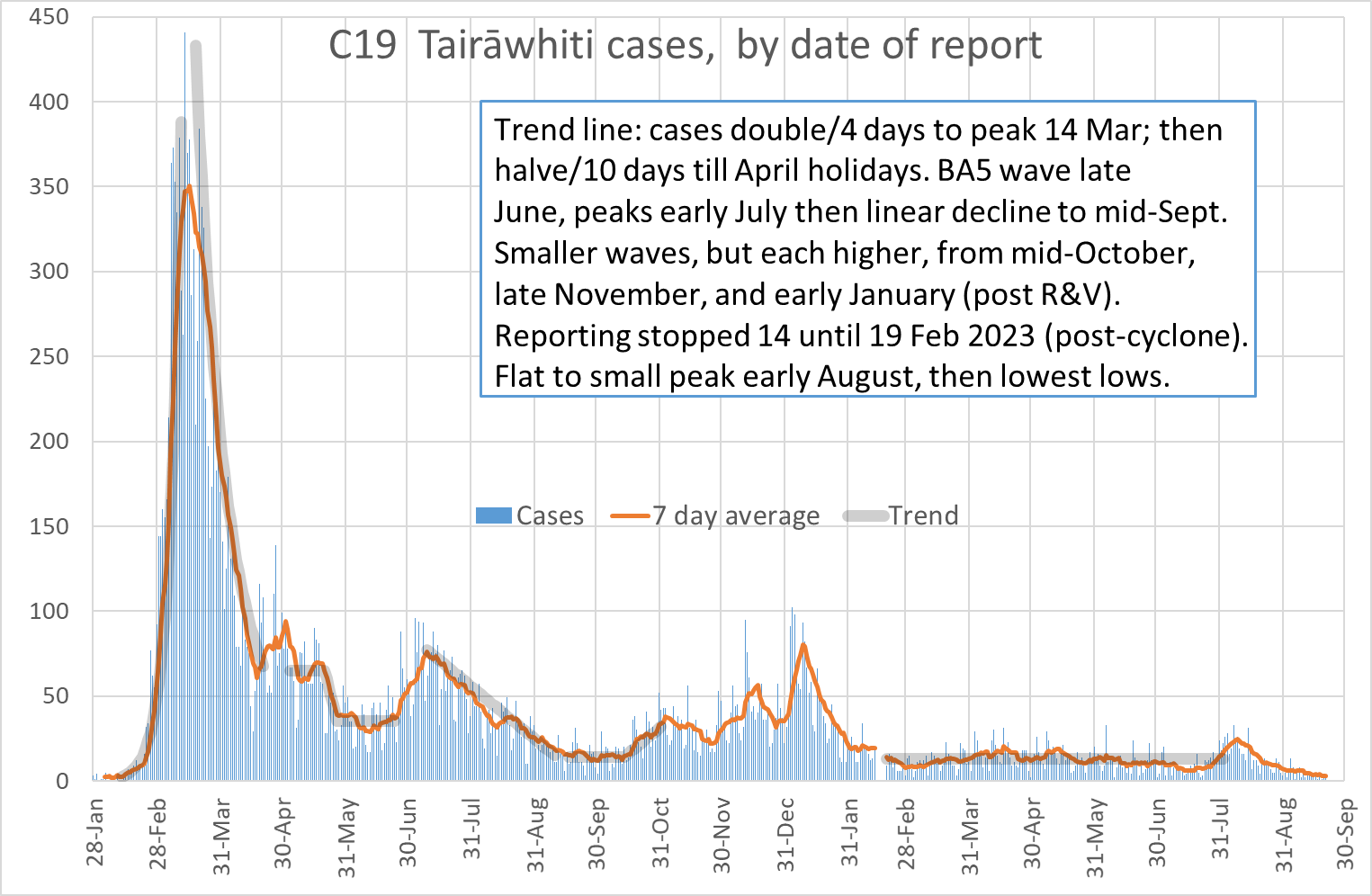
Daily case count for Friday to Thursday: 3, 5, 1, 5, 1, 2, 3 compared to 8, 2, 5, 2, 5, 4, 3 for last week. This week, all cases were diagnosed by RAT (self-reported). No Covid hospitalisations this week; compared to two last week. The last hospitalisation was on 12 September.
Under-testing and reporting, following the drop of all mandates on 15 August, means that the reported numbers are likely a smaller fraction of all infections. But wastewater data shows decrease with the drop in cases for week ending 17 September:
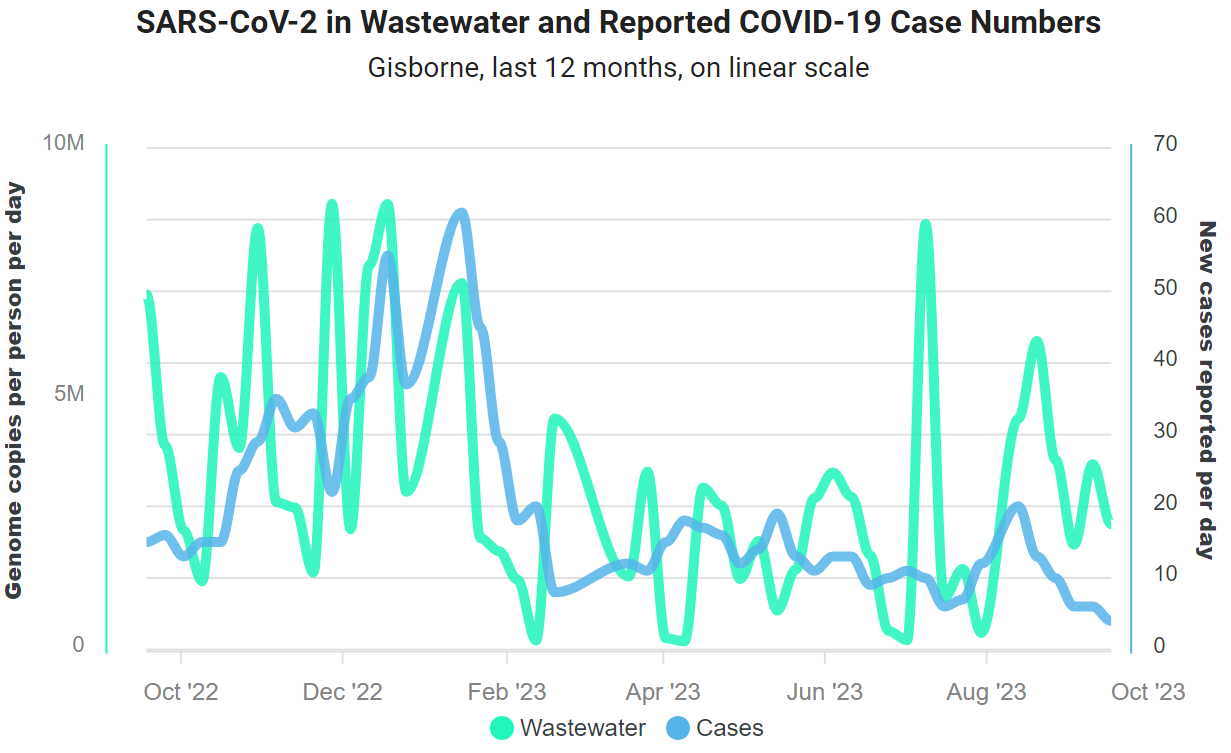
The previous week wastewater levels increased, despite a nearly flat case line. I suggested that may reflect noise or increased under-reporting. Contributing to ‘noise’ is the variable level and duration viral RNA excretion from each case.
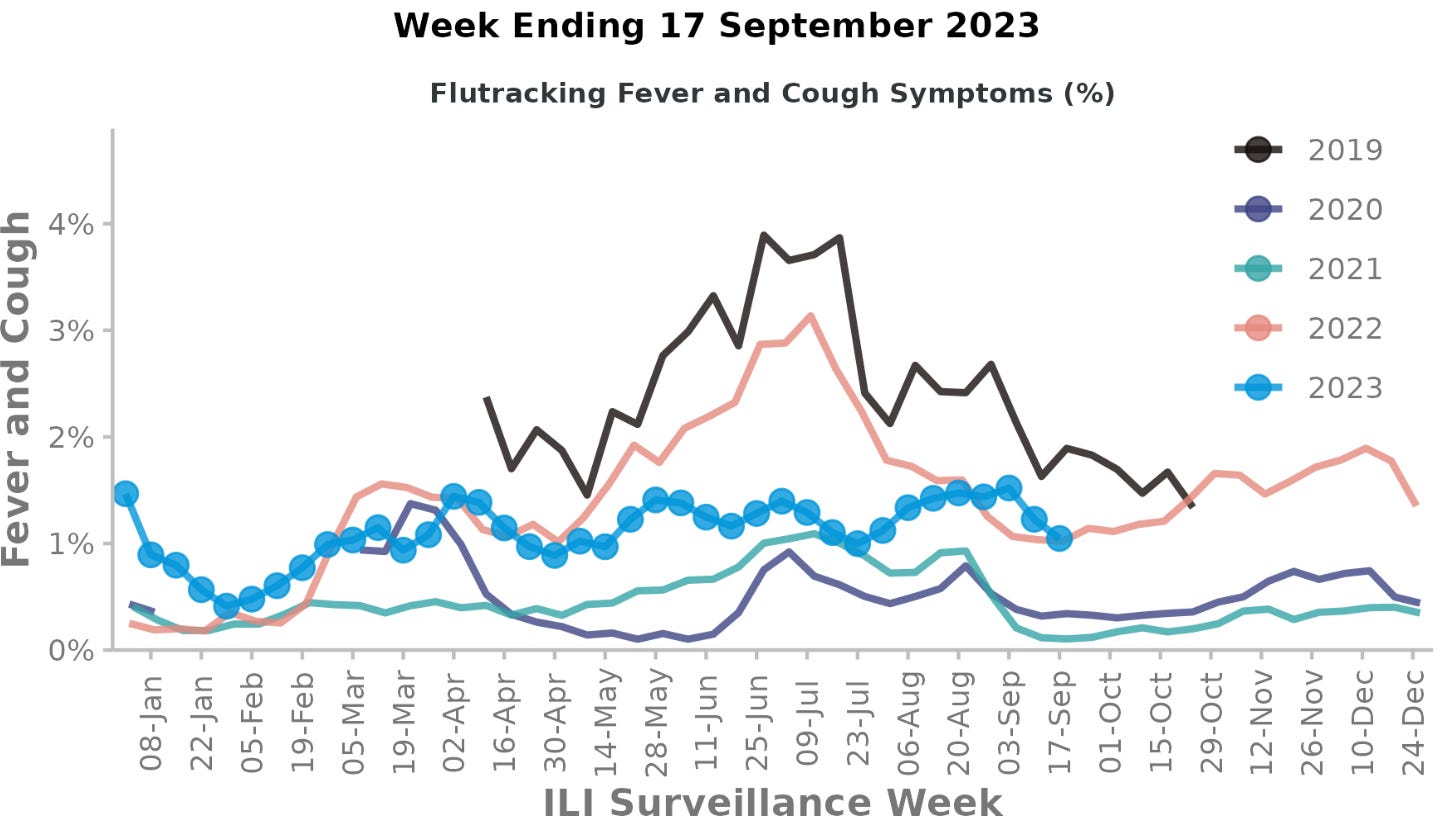
National acute respiratory illness surveillance for the week ending 17 September showed continuing decreases in illness. The previous week, hospitalisations for respiratory infections had increased despite lower community illness; this week hospilalisations declined to ‘moderate’. FluTracking found lower rates of symptoms:
Typhoid cluster
Last week, I wrote about a possible typhoid cluster. There are now five confirmed cases, including the likely source: the cook for this group of close-living workers, was an asymptomatic carrier. There have been no cases outside this group.
Most of the 16 contacts have now returned negative stools, though three were positive for Campylobacter. As they had no symptoms, and asymptomatic infection with Campylobacter is rare, it may reflect recent infection as PCR is very sensitive.
Other notifications
One other Campylobacter notification, with no potential source identified. Like most enteric infection notifications, there were no others in the household or contacts with any illness. It seems unlikely that others were not exposed to the source, but it is possible as only a few of these organisms are needed to get infected.
And a case with a dual enteric infection: Giardia and Shiga Toxin-Producing Escherichia coli (STEC). I previously wrote about STEC, that can cause lead to a life-threatening complication from kidney damage and/or clotting. Again, no others in the household or contacts who were unwell. Of note, the case has been unwell since getting Covid last month.
Leptospirosis tests
Last week, we awaited a second blood test to confirm for the leptospirosis case. The results confirmed the diagnosis. The responsible serovar (the subtype of the bacterium) was Hardjo that is usually found in cattle, confirming likely exposure from working at an abattoir (‘meat works’).
Leptospirosis is hard to diagnose clinically or by lab test. Let me explain the tests.
Comparing the immune response during the illness (‘acute’) and afterwards (‘convalescent’) was often used to test for specific infections, before we had PCR. The PCR test is usually very sensitive at detecting nucleic acids (DNA or RNA) that identify the organism. Nowadays, PCR is generally the preferred test (eg, Covid, measles, pertussis, enteric infections).
But PCR tests are not so sensitive in leptospirosis. A NZ study found that 36% of cases were not detected by PCR, even early in illness. The PCR test can be done on blood or urine. The same NZ study recommends testing both urine and blood with PCR, in addition to the immune response. (The latter also identifies the serovar - or subtype.)
The IgM test can be negative in the first few days (when blood PCR is more likely to be positive), but is usually very sensitive and used as screening test because it can be positive from other infections. If IgM+, a special test of immune response, to leptospirosis is called the microscopic agglutination test (MAT), is used that also identifies the serovar. For the MAT, an acute and convalescent sample are needed to see a rise in response; though a very high response on the first test (≥ 400) is diagnostic.
In our case, the acute sample did show an elevated level to Leptospira Hardjo, but at 200 this would be suggestive (‘probable’ case); a level of 400 would have confirmed the diagnosis. The second sample level rose to 6,400, confirming the diagnosis with greater than four-fold rise. The other 7 serovars tested stayed at or below 25.
Next week
Is it time to stop the weekly reporting of Covid cases? As always, look forward to your feedback and suggestions; and any questions on the data. Thank-you!
Kia ora Oz, great discussion on lepto tests and neat to see you delving deep into local data.