
Tairāwhiti data, 21 July 2023
Tairāwhiti data, 21 July 2023
Notifications in the past week; focus on invasive pneumococcal disease

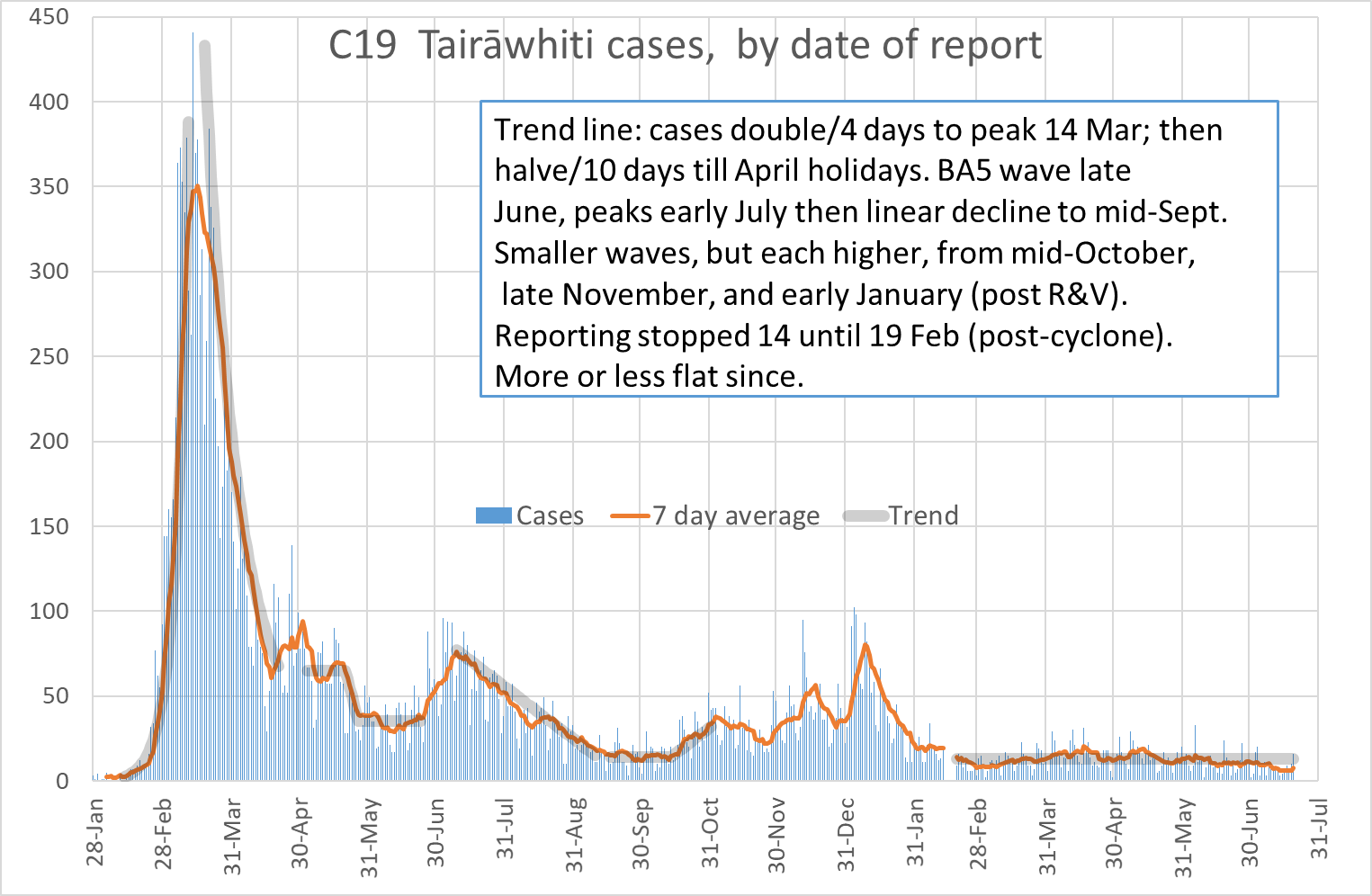
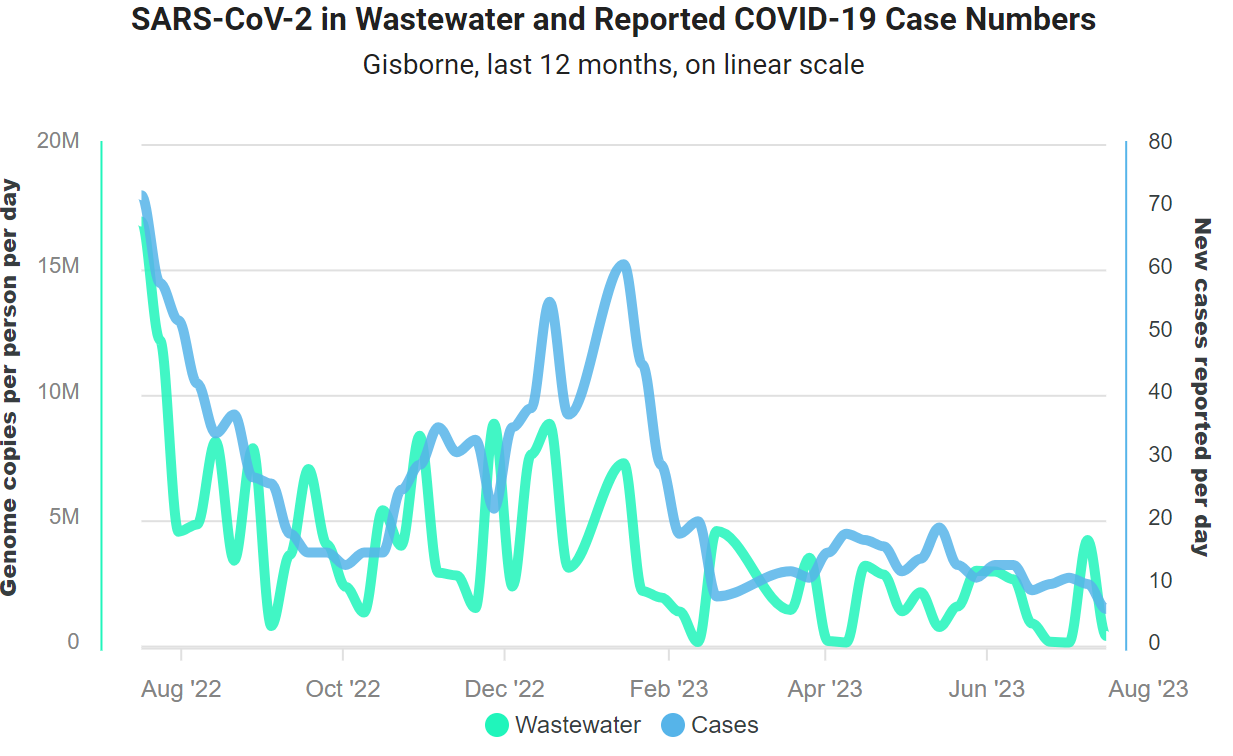
School term started on Monday, and we have a small rise in Covid notifications from 3 last Friday to 16 yesterday. The 7-day average remains just over 7 cases per day. No hospital admissions with Covid since 9 July, in line with lower case notifications. Wastewater data to 16 July show a drop last week (chart below). Nationally, cases and wastewater declined last week.
National surveillance for respiratory viruses has not yet been updated for the week ending 16 July; so far have been at low rates for the time of year with influenza the main virus. Not too late to get an influenza vaccine as the circulating strains have been showing a good match. Especially important for those with medical conditions like diabetes and heart disease; and those who live with them.
Other notifications
Other notifications in the past week: one Campylobacter and one invasive pneumococcal disease. Campylobacter remains the most commonly notified infection except for Covid. Last week, I reported on enteric notifications for the first two weeks of July: 5 cases of Campylobacter. And shared the April 2023 report on enteric infections, with a focus on STEC and Yersinia. Thanks for any comments!
Gonorrhoea
We also had a query from a clinician about reporting a case of gonorrhoea. Three sexually-transmitted infections (HIV, syphilis, and gonorrhoea) are notifiable, but each one has a different process and all three ask for anonymous notification. The gonorrhoea notification process is outlined here. The person’s name is not reported, but notification asks for their demographic details, testing information, and risk factors including sexual behaviour. I will report our STI data at some stage; we have been the district with the highest rates of gonorrhoea.
Invasive pneumococcal disease (IPD)
The national immunisation schedule offers protection against 16 diseases. These diseases are notifiable to monitor outcomes, except for varicella (chickenpox), shingles, influenza, and rotavirus (except as cause of outbreak).
Pneumococcal conjugate vaccine (PCV) was added to the national immunisation schedule for children in 2008, and the disease made notifiable later that year. For pneumococcal disease, the primary purpose is to monitor serotypes. Let me explain.
First, conjugated vaccines. These conjugate (or bind) a protein to the polysaccharide (chain of sugars) that coats the bacterium. The polysaccharide is the key antigen - the target of our immune response. Children under the age of two years do not mount an immune response to polysaccharide alone, but do so when it is bound to a protein.
This was first demonstrated with Haemophilus influenzae type b (Hib). When Hib was added to the NZ immunisation schedule in 1994, it was the most common cause of life-threatening bacterial infection in children aged under 5 years. Since introduction, nationally and globally, Hib disease has been practically eliminated.
The pneumococcus is the short name for the bacterium Streptococcus pneumoniae. It is part of the ‘normal flora’ living on the surface of our upper airways. But when it invades the surface it causes serious diseases, mainly meningitis and sepsis; or it can spread to the lungs to cause pneumonia.
A serotype refers to a distinct strain of the microorganism, based on serological (antigen) testing. For pneumococcus, over 100 different serotypes have been progressively identified. The risk of disease and its severity varies by serotype; antibiotic resistance is also more common in some. In general, most invasive disease is caused by only a few serotypes.
The first pneumococcal conjugate vaccine (PCV) included seven serotypes (PCV7). We moved to PCV10 in 2011 and PCV13 in 2014, then back to PCV10 in 2017. The serotypes covered by each vaccine:
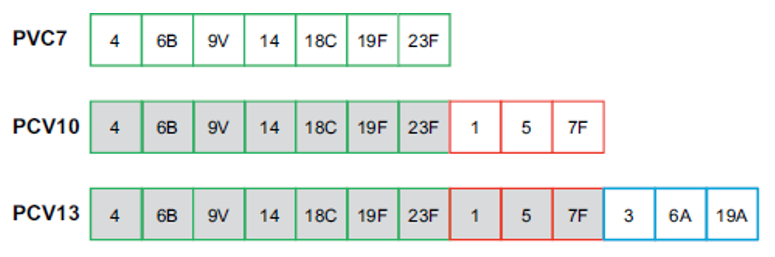
The concern that vaccine serotypes would be replaced by serotypes not in the vaccine has been partially proven. So, we need to monitor the serotypes causing invasive disease. There has indeed been some evidence of replacement in international data, with variable impacts but overall not leading to much loss of vaccine impact.
Hence, the need to to monitor the serotypes causing invasive pneumococcal disease (IPD). As a result of our monitoring, we reverted to PCV13 in 2022 as the 19A serotype was on the rise.
Local IPD notifications
The chart of IPD notifications in our district shows moderate year-to-year variation, and progressively more Māori cases, especially 2021:
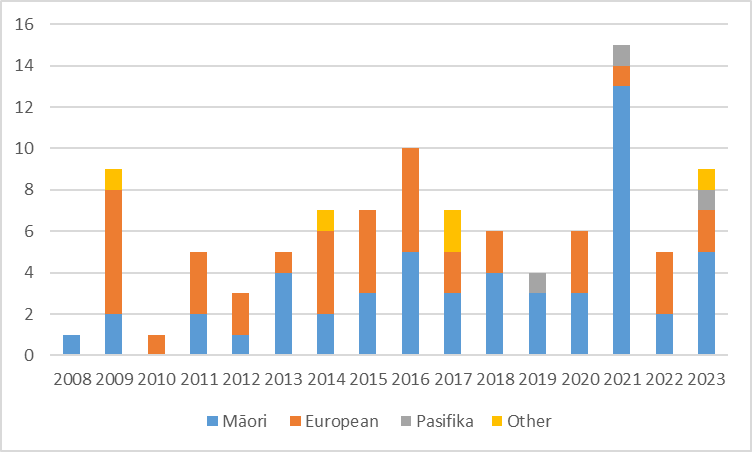
About half of our population is Māori, about 5% Pasifika and another 3% or so in other groups. However, the European population has an older age profile that increases the risk of IPD. Only 11 of the 100 cases were aged under 5 years.
Next week
We may see more impact from school term 3 starting this week, as schools are an important source of spread in the community. Hopefully, we can keep at our low level of disease notifications. Perhaps we can talk about sugary drinks?
As always, look forward to your feedback and suggestions; and any questions on the data. Thank-you for reading!
Ngā mihi & Kind regards, Oz