
Scabies: The Itch
A neglected communicable disease that needs more attention to address an important and possibly growing health burden. And early warning for winter infections; measles imports.

My weekly Monday missive is late. We had few notifications last week, so I thought to share some of what I have been learning about a neglected health risk: scabies.
It took longer than I planned. And got sidetracked by measles imports and winter preparedness with what may be a warning for an early influenza season.
Respiratory infections on the rise and winter is coming…
Influenza has been called ‘predictably unpredictable’ as each winter season has a different pattern. Our Emergency Department (ED) kindly informed me of cases positive for Influenza A over the weekend. And Covid.
I have noted the increase in Covid hospitalisations over recent weeks, and last week also showed the rise in wastewater levels. (Data to 1 March charted in link. And no hospitalisations since)
On radio on Monday, Michael Baker described the recent increase in Covid hospitalisations and wastewater nationally. He suggested that loss of immunity in the vulnerable with low uptake of boosters and the limited duration of vaccine or virus immunity. That’s plausible if vaccine immunity is more protective against severe disease than previous infection.
We continue to see studies showing the effectiveness of a recent booster. For example, this recently published US study found a vaccine effectiveness ( VE) of 40% against hospitalization and 79% against invasive mechanical ventilation or death - if received within the previous 3-6 months.
Not nearly as effective as measles vaccine that gives essentially lifelong immunity (with some initial failures and some later ones as immunity can wane). The Covid vaccine offers good short-term protections, but not the near perfect of >95% with measles vaccine. But to maintain that good protection, you needed regular boosters. Is that still the case? I would expect so, as the studies continue to show the protective effects of recent boosters. But of course, we can only know the past.
The influenza vaccine will be offered from 1 April. The updated Covid vaccine is already available. Let’s see if the data confirm an early influenza season and if Covid has peaked. If you are at increased risk because of your age or medical conditions, do get both vaccines.
Measles back in NZ
We also had yet another measles import reported, bringing us five new measles cases in 2026. The five cases were in four events, as two of them were together when infected. Here I list the date of Health NZ’s report (and location of case) and URL:
29 Jan 2026 (Tauranga): https://www.tewhatuora.govt.nz/news-and-updates/new-measles-case-in-tauranga
24 Feb 2026 (Auckland): https://www.tewhatuora.govt.nz/news-and-updates/two-new-measles-cases-confirmed-in-auckland-linked-to-overseas-travel
27 Feb 2026 (Auckland): https://www.tewhatuora.govt.nz/news-and-updates/new-measles-case-confirmed-in-auckland-linked-to-overseas-travel
06 Mar 2026 (Wellington): https://www.tewhatuora.govt.nz/news-and-updates/auckland-international-airport-a-location-of-interest-after-new-measles-case. And on 8 March: https://www.tewhatuora.govt.nz/news-and-updates/more-measles-locations-of-interest-confirmed-public-asked-to-monitor-for-symptoms
The reports do show that the first and last were visitors and the other three were returning travellers. But not the date of rash onset, except for the first case; nor the likely country where they were infected.
So far, no spread has been detected from any of these imports. We are still within the 3-week interval since from the infectious period of the most recent cases. But past the median incubation period. So, if there is spread, it will likely be limited.
From 2023 to 2025, there were at least 12 measles imports. For only five of these was there any spread. And that spread was limited, except the import that started the September 2025 Northland outbreak with that virus spreading until December 2025.
So, we still remain measles-free, despite the warnings of an impending massive measles epidemic.
Scabies
In last week’s report, I included this short explanation of the disease adapted from the World Scabies Program:
Tiny female mites burrow into the skin and lay eggs.
Mites cause papules and an intense itch, worse at night.
Typical burrow locations include fingers toes, wrists, buttocks and genitals.
Spread is person to person, primarily through direct skin-to-skin contact.
Spreads easily in crowded conditions; schools, childhood centres and prisons.
Infected skin sores (impetigo) can result in life-threatening conditions, including rheumatic fever.
Today, let’s get into the details of these points. This was to lead us to a muse on the role of the National Public Health Service (NPHS) and the health system in addressing this neglected communicable disease. But this post was already too long, so will come back to these issues later; but keen to get your thoughts on how to deal with this neglected disease of public health importance, that is not addressed as other communicable diseases by the NPHS.
Tiny female mites burrow into the skin and lay eggs
The scabies mite, Sarcoptes scabiei, is a microscopic (<0.5mm length), eight-legged parasite. It is too small to be seen by the naked eye, except possibly as a small dot.
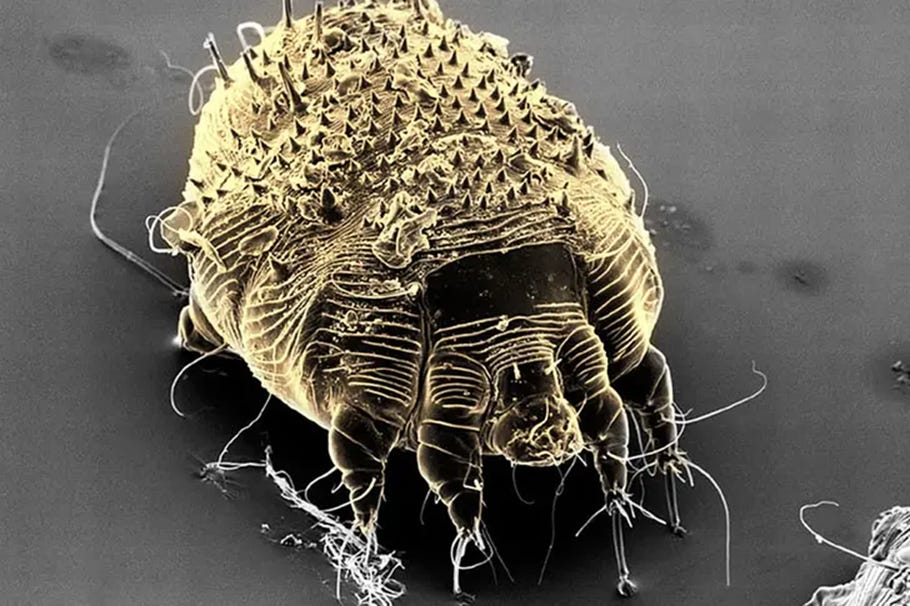
The mite has adapted to different hosts. The human variant (Sarcoptes scabiei var. hominis) lives only on human skin. Animal variants do not usually infest humans; but can occasionally infect humans, but the animal mites cannot reprodue on human skin so it does not spread. The fact that humans are its only host, like smallpox, makes this parasite potentially eradicable.
The mite’s life cycle is shown in this image; that also shows the superficial layer of skin (stratum corneum) where the pregnant female mite burrows to lays its eggs:
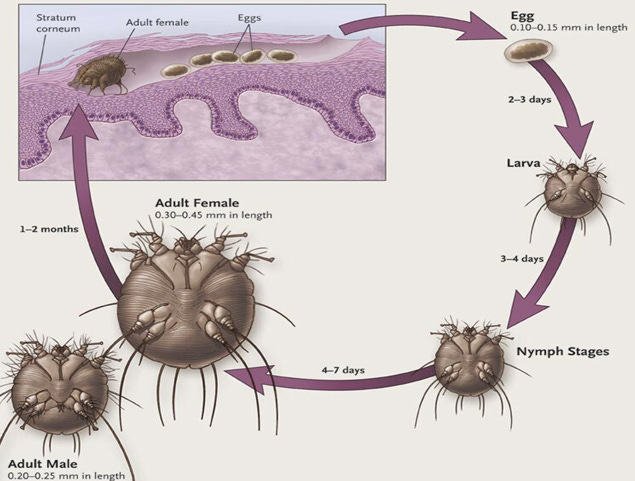
The pregnant female burrows between 0.5–5 mm per day, laying ~1-3 eggs daily for its lifetime of 4-8 weeks. The eggs hatch in 2-5 days - note the image above states 2-3 days, CDC states 3-4 days, and DermNet states 2-5 days. The last is most credible I did not find a Health NZ estimate; and is from NZ.
Conflicting data is an issue with scabies. Some variation may be due to different temperature, humidity, or other conditions. It also reflects the limited data on this neglected disease; much based on laboratory studies of non-human variants.
One review notes the length of the mite’s lifecycle reported as: 12-17 days, 17-21 days, 7 to 10 days, 9 to 15 days and ‘about 15 days’. The duration matters, especially the time for eggs to hatch as the treatments do not kill the eggs, and so the second treatment needs to be after the mites have hatched but before they reproduce and make new eggs. So, the second treatment is recommended 7-14 days after the first; seems safer to use 7 days when all the eggs are hatched.
Upon hatching, the larvae migrate from the burrow to the skin surface. There they find a hair follicle or skin groove to create a ‘molting patch’. This is a very short burrow where the larvae grow and molt. The lave molts into two nymph stages; and the final molt is to become adult. The adult male mite seeks the female in its molting patch and dies after copulation. The female only has sex once and leaves its molting patch to find a suitable part of skin to burrow into. And there starts laying eggs. And so the cycle continues.
Interesting side notes: larvae have six legs; nymphs (and adults) have eight legs. The mite does not mechanically burrow into skin cells, but dissolves them.
Mites cause papules and an intense itch, worse at night
Our bodies’ immune reaction to the mite takes time to develop. Usually 4-6 weeks, but can be to 2 months and possibly as short as 3 weeks. The reaction leads to itch and papules - a small red lump that are both generated by the body’s reaction to the mite. Not to the mite itself, but its waste products.
Unless previously infested, when the itch will appear ‘within hours’ (DermNet) or in 1-4 days (CDC).

The itch is characteristically worse at night. Being woken by itch suggests scabies. Hypothesized as being due to increased mite movement. The itch is not related to the presence of the mite itself, but its waste products that our immune system reacts to. So, the site of scratching may no longer have any scabies mite.
The burrow is the hallmark of scabies. These are '“curvilinear or serpiginous thread-like tracks measuring around 5–10 mm”. But papules and vesicles as well as itching will often obscure it. In addition, there can be a general eczematous eruption on the torso and limbs that obscures the papules and burrows.
Itching can lead to breaks in the skin that allow bacterial infections that can be serious. These include impetigo, cellulitis, sepsis, and other complications. Group A Streptococcal infection can lead to kidney damage and acute rheumatic fever (ARF). A NZ study found a strong association between scabies and ARF.
The itch is not mediated by histamine. So anti-histamines are of limited value. Nevertheless, they can help perhaps from the secondary effects of the itching; sedating anti-histamines are useful at night.
Crotamiton cream is both anti-mite and anti-itch. Not as effective as permethrin, but can be used in addition to permethrin or ivermectin for itch symptoms.
Typical burrow locations include fingers toes, wrists, buttocks and genitals
DermNet details: “Lesions are symmetrical, and mainly affect the hands, wrists, axillae, thighs, buttocks, waist, soles of the feet, areola and vulva in females and penis and scrotum in males. The neck and above are usually spared, except in cases of crusted scabies and in infections occurring in infants, the elderly, and the immunocompromised.”
I like this graphic from a review that shows locations and types of lesions:
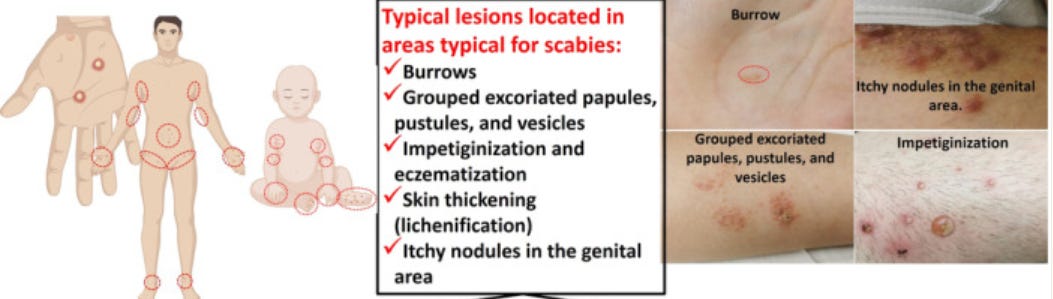
The burrows are typically identified in the web spaces, palms, soles, fingers, toes, inner wrists, elbows, umbilicus, and beltline.
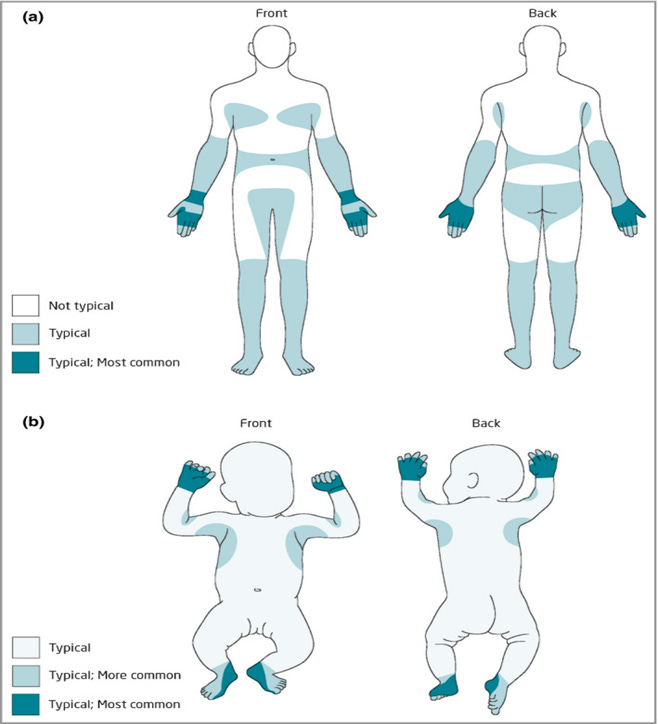
The 2020 International Alliance for the Control of Scabies Consensus Criteria for the Diagnosis of Scabies includes this image of the typical distribution of scabies lesions for those (a) Age > 2 years (b) Age < 2 years.
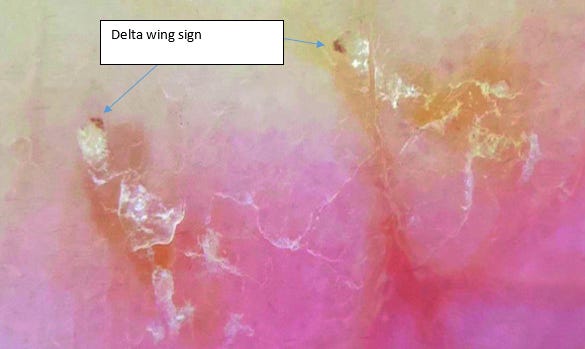
Dermoscope (or dermatoscope) provide magnification that enable visualisation of the mite that looks like a Delta wing at the end of the burrow:
Burrows can be visualised without magnification by the ink test:
Apply ink from a non-toxic water-soluble felt tip pen over the suspected entrance of the burrow. Wait a few moments and then wash off the ink. The ink will track down a scabietic burrow forming a characteristic dark zig-zag line.
Spread is person to person, primarily through direct skin-to-skin contact
As we noted, the human variant of the scabies mite can only live on humans, and dies quickly if not on human skin. So, it can only spread person-to-person. As the mite cannot fly or jump, it needs direct skin-to-skin contact to spread.
This requires at least a few minutes of contact. And can be washed off before it has time burrow. But this can happen in as little as 20 minutes. Washing will remove it before it has the chance to do so.
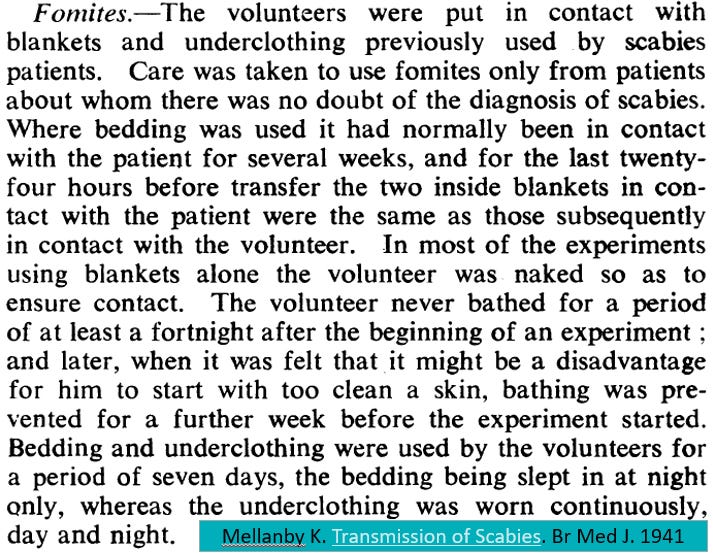
The mite can also spread through infected bedding or clothes. But these are more likely to lead to re-infection than infecting others. During the second world war, Dr Kenneth Mellanby used conscientious objectors to see how well the mite could be transmitted. In 63 experiments using bedding and clothing of a scabies patient, there were only two transmissions; and none with bedding alone. The two transmissions were from 32 who wore underclothes immediately after being worn by a scabies patient. None were infected when the underclothes were not worn for 2-7 days after being worn by the scabies patients. This was in contrast to the easy spread from skin-to-skin contact. You might enjoy this description from his 1941 article:
The mites need to be on human skin to survive and die from dehydration when not on skin. Usually within a a day or two. Survival is commonly quoted as 24-26 hours at 21oC and 40-80% relative humidity. But dehydration will be slower in cold and humid conditions, and possibly lasting up to a week. Though most guidelines suggest that 3 or 4 days is enough.
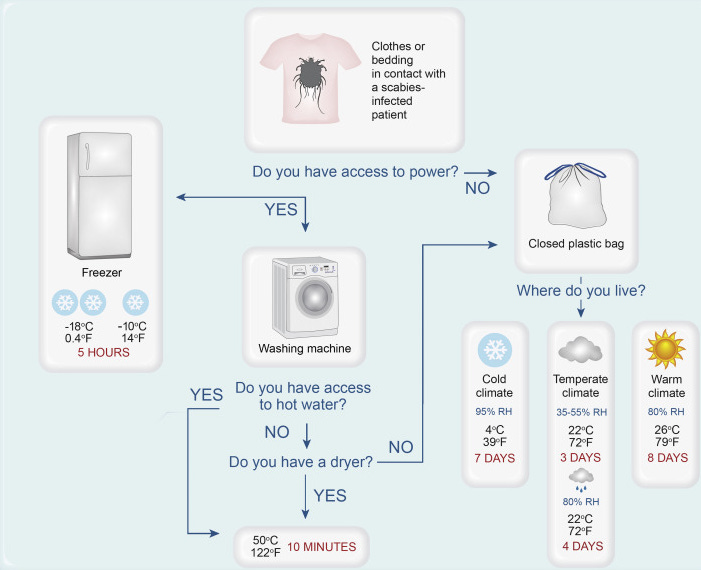
An Australian study using the pig variant found that all mites and eggs were killed at a temperature of 50oC after 10 minutes. And that it took at least 3 days for all the mites that are bagged to die, but it can be up to 7 days at low temperature and high humidity.
Based on that study they developed this useful flow chart:
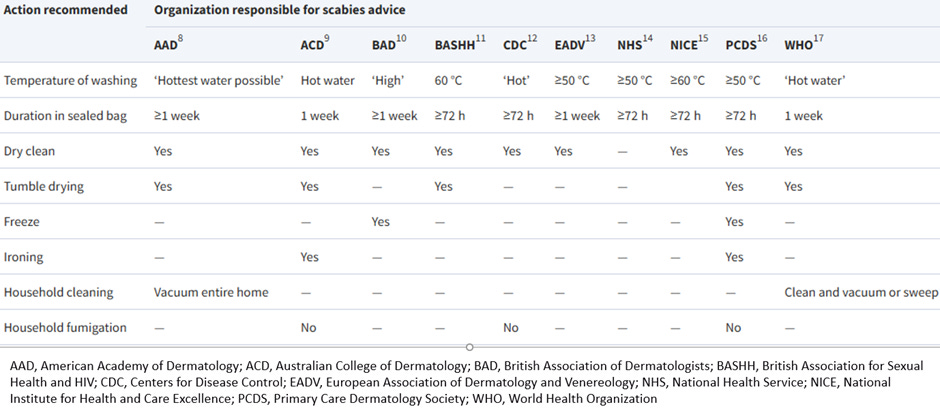
But a Thai study using the human variant found that it took 35 minutes at 50oC to kill all mites and eggs. There may be more data on the issue, but the variable guidance was shown in this review of online resources:
History
Scabies is an ancient scourge. The earliest reference to scabies may be from ~1200 BCE in the Bible (Leviticus 13:8). Aristotle described scabies as “lice in the flesh”. In 25 CE, Aulus Cornelius Celsus named the disease from Latin ‘scabere’ - to scratch.[Scabies was also called ‘The Itch’.
“James (VI) King of Scotland, and later England, was reported to have said that ‘None but kings and princes should have The Itch for the sensation of scratching was so delightful’. In my experience, few sufferers of scabies would agree with this description.” Craig E. The Itch: Scabies. Oxford, 2022.
Thomas Moffett was the first to identify the scabies mite as distinct from the louse in the 16th century. With the advent of the microscope s details could be seen and was first drawn in the 17th century by August Hauptmann and Michael Ettmüller. The recognition of the relation of disease to mite was first recorded in a 1687 letter entitled, “Observations concerning the fleshworms of the human body” by Giovanni Bonomo (with Diacinto Cestoni) who described extracting the mite from the burrow of several patients with scabies.26 These observations predated germ theory by two centuries, and may be the first demonstration of a micro-organism causing disease.
In 2017, scabies was added to the World Health Organization (WHO) neglected tropical disease (NTD) list in 2017 because of its high disease burden. The Global Burden of Disease (GBD) Study estimated that in 2021, “scabies caused 5.3 million DALYs, 206.6 million prevalence, and 622.5 million annual incidence, primarily affecting children and young people.”
Our involvement
During 2025, we received requests to support households with treatment failure. An essential aspect of treatment is to treat all household and other close contacts (within past two months) at the same time with anti-scabies cream or medicine.
Through these referrals we identified these barriers to correct treatment:
Lack of understanding and knowledge gaps
o Overwhelmed by instructions, hard to organise everyone
o Stigma - families feel judged, whakamā, mental health, exhausted
o Don’t know where to turn for help and frustrated with persistent itch
o Not understanding the severity/risks to whanau if left untreated
Inadequate laundry facilities and spare bedding
o Laundry costs as unable to wash at home ($150 each time for one household)
Lack of spare bedding/clothes
Costs for GP visits and medication, including transport cost
We also found that the patients had been given variable advice by different health practitioners and important inconsistencies in the available health information material. (Prompting the new NPHS information resource issued in December 2025.)
Next week
I will continue on the issues around treatment for scabies, and what it tells us about our health system. Or give you the data update and continue with scabies at a later date.
As always, look forward to your feedback and suggestions; and any questions on the information shared. Thank-you for making it to the end!
A damn fine overview of scabies. I can see why it took you some time to put together :)